Patient scenario
2month old Caucasian female, with no significant medical history, presents to the office with her mother and father for her 2month well exam and vaccinations ( HIB, DTAP, rotavirus vaccines). Mom states the child has been feeding and growing well, however she has been worried about her baby because “she is very fussy and spits up a lot”. She explains the child spits up 4-5 times a day, after feeds, and sometimes turns blue in the face. The child also becomes stiff with her back arched during these episodes. She has had four episodes in the past month and usually returns to normal within a 1-2 mins after the episode subsides. Mother reports two of those episodes consisted of projectile vomiting both occurring after her nighttime feedings, but on different days. Mom also explains the baby cries a lot after feeds and wants to be held and backwards positions where her arms are wrapped around the child’s stomach. She claims the baby appears to be more comfortable in this position. Patient is on Enfamil infant formula and drinks about 4 ounces of formula every 3-4 hours. Mother denies the baby has had any, diarrhea, blood in the stool, weight loss, coughing, feeding refusal, wheezing or signs of lethargy.
Patient is exhibiting signs of Reflux.
Diagnosis and Treatment of Gastroesophageal Reflux in Infants and Children.
American Family Physician is a biweekly peer-reviewed medical journal published by the American Academy of Family Physicians. It provides continuing medical education for family physicians and other primary care clinicians.
This article was a 2015 Review article which conducted:
- PubMed search using the key terms reflux, gastroesophageal reflux, and gastroesophageal reflux disease, limited in children age 0 to 18, and combined in separate searches with epidemiology, etiology, pathophysiology, diagnosis, management, and treatment for reflux related topics, including clinical reviews, randomized controlled trials, systematic reviews, and meta-analyses.
- Other databases searched included: Cochrane Database of Systematic Reviews, the National Guide- line Clearinghouse database, and Essential Evidence Plus.
- In addition, a search was conducted using individual diagnoses within the differential diagnosis of reflux as key terms, limited in children age 0 to 18, and combined in separate searches with etiology, diagnosis, management, and treatment.
- Relevant publications from the reference sections of cited articles were also reviewed.
- Search dates: January through July 2014, and February and July 2015.
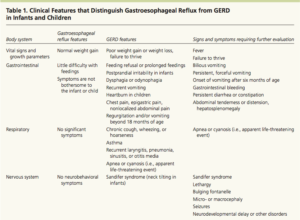
Article emphasizes that the following should be kept in mind when dealing with regurgitation and projectile vomiting in a child.
- Progressively worsening projectile vomiting in the first months of life is concerning for pyloric stenosis and requires immediate imaging and surgical referral.
- Recurrent non-projectile vomiting or regurgitation beyond 18 months of age is uncommon and suggests GERD or more concerning pathology so requires attention.
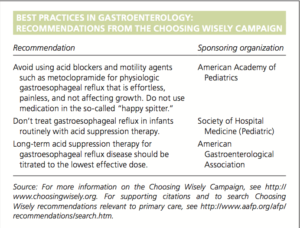
Recommendations made by article:
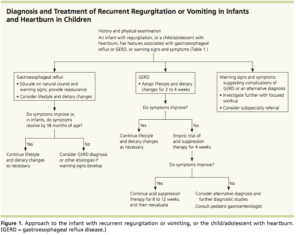
- The diagnosis of Gastroesophageal reflux and GERD should be based primarily on history and physical examination findings, because other diagnostic tests have not shown superior accuracy. (see algorithm below)
- Conservative treatments are the first-line strategies for most infants, older children, and adolescents with reflux and GERD.
Conservative treatments:
Infants:
- Reduce feeding volumes and offer more frequent feeds
- Change the infant’s body position after feedings, while awake and observed. Prone and left side down positions shown to decrease reflux episodes.
- Adding thickening agents (i.e., 1 tbsp rice cereal per oz of formula) decreases observed regurgitation and esophageal regurgitant height, but does not reduce the reflux index (percentage of time the esophageal pH is less than 4) and can lead to excess weight gain.
For adolescents:
- Avoid alcohol
- Weight loss in those who are obese
- Smoking cessation
- Chewing sugarless gum after meals,
- Avoid late evening meals
- Sleeping with the head of the bed elevated or in the left lateral decubitus positions.
- A trial of extensively hydrolyzed or amino acid formula in formula-fed infants, or maternal dietary modification in breastfed infants, is warranted when reflux is presumed to be caused by an allergy
to cow’s milk protein. - Histamine H2 receptor antagonists are an option for acid suppression therapy in infants and children with GERD.
- Proton pump inhibitors are reasonable treatment options for GERD in older children and adolescents, but their use in infants is questionable because of a lack of proven effectiveness.
- Provides excellent chart about the pros and cons of diagnostic testing in GERD. (See below)
- Provides insight on surgical treatment options and explains limitations which consist of reflux recurrence.
- Type of surgery performed -Complete or partial Nissen fundoplication
- Article also covers different type of H2 antagonist and PPIs and their effectiveness and cost effectiveness.


This entry is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International license.